



TPLO treatment of anterior cruciate ligament rupture in dogs and cats
Anterior cruciate ligament (CCL) injuries are defined as partial or complete ruptures of the ligament, or tears at its origin or insertion. The cranial drawer test describes excessive anterior-posterior translation of the tibia relative to the femur following CCL injury. Cranial tilbial thrust (CTT) refers to anterior translation of the tibial tuberosity in the knee joint with ACL injury when the tarsal joint is flexed and the gastrocnemius muscles contract. Tibial plateau leveling osteotomy (TPLO) alters the mechanics of the knee joint, achieving stability through active joint restraint [1.2]. The goal of TPLO surgery is to create a tibial plateau slope (3-7 degrees) that effectively controls tibial sliding by actively restraining the posterior cruciate ligament and the knee joint. TPLO is an effective surgical procedure for dogs with complete and partial CCL ruptures.
Principles of TPLO surgery:
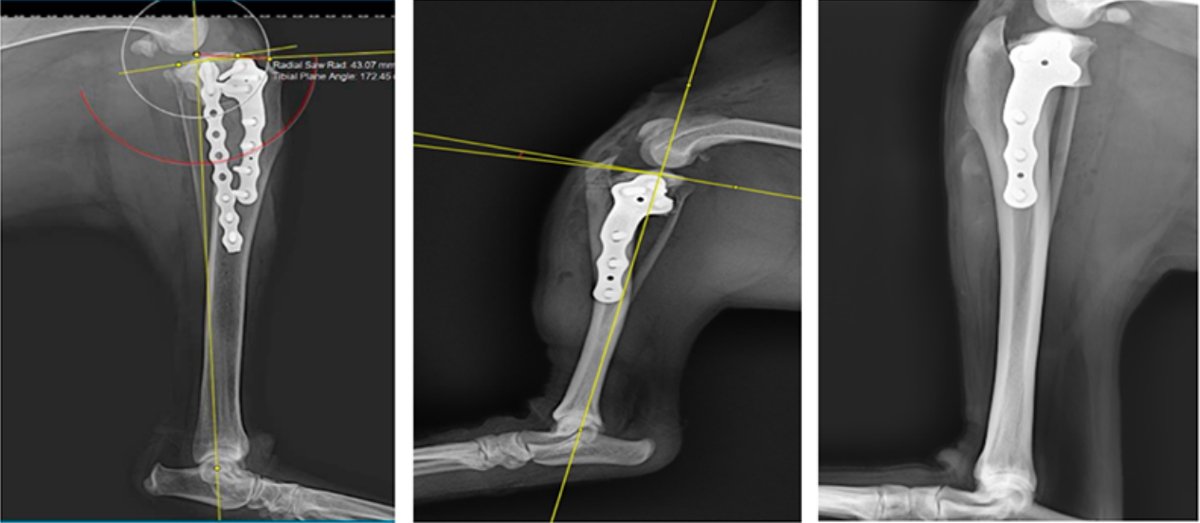
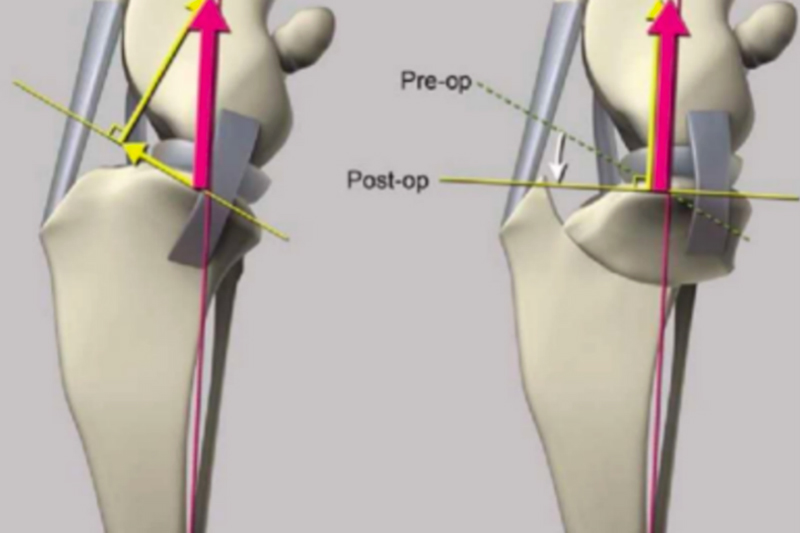
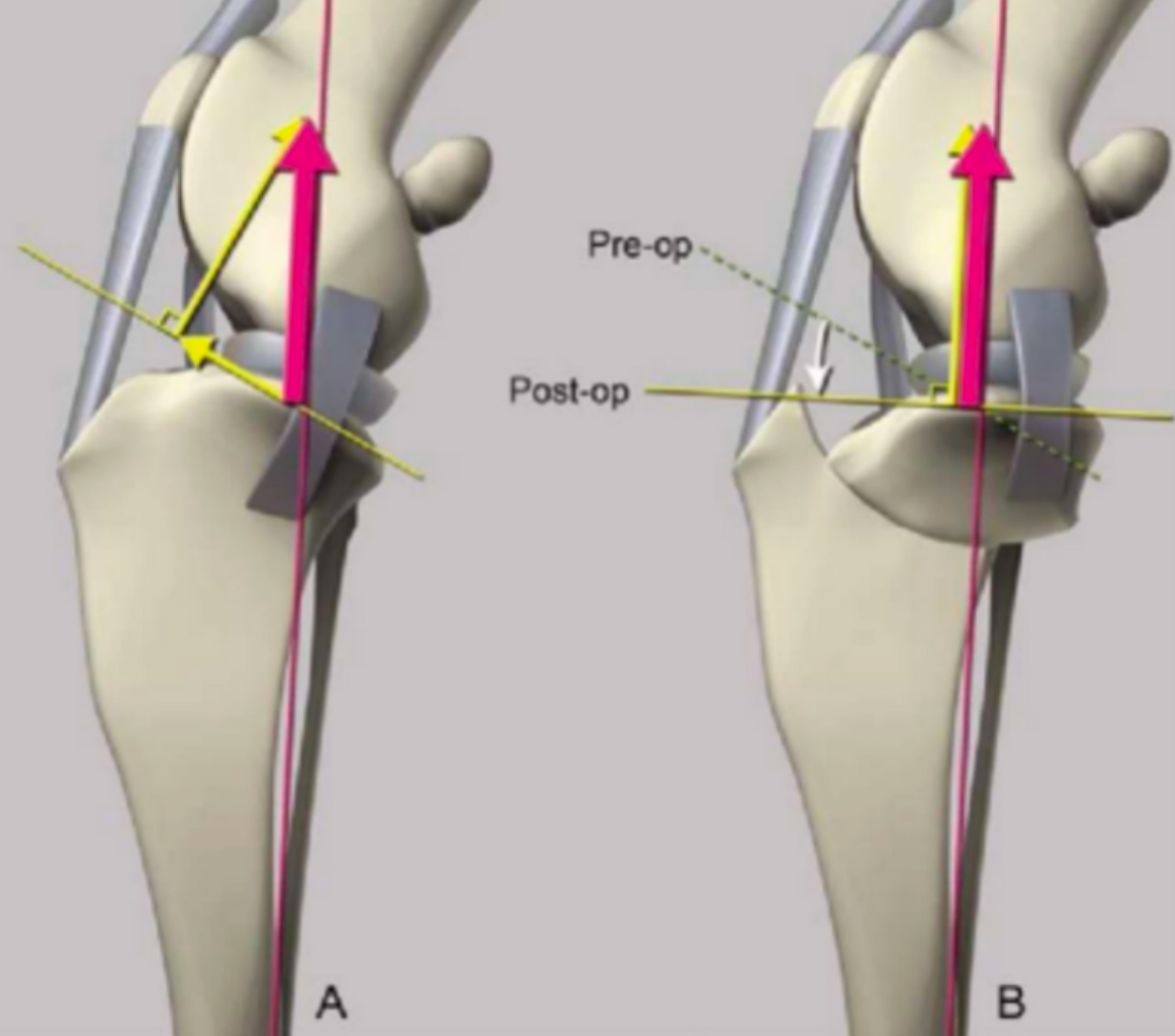
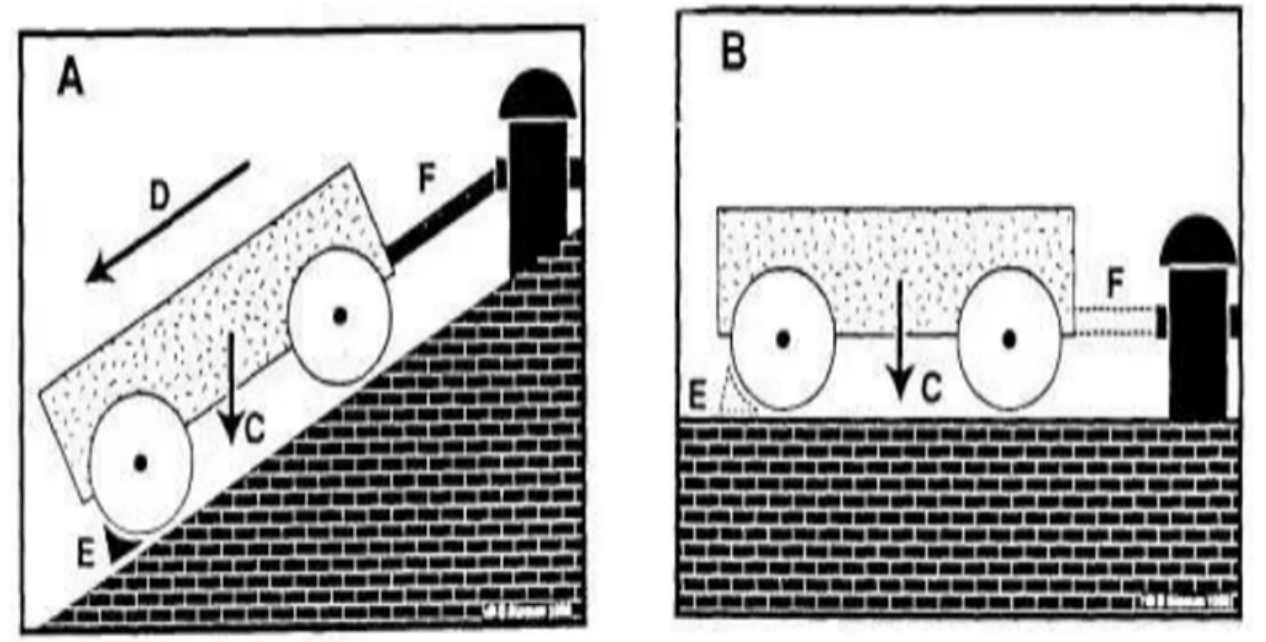
Tibial plateau leveling osteotomy (TPLO) alters the mechanical structure of the knee joint, achieving stability through active joint restraint [1.2]. Because the tibial plateau has a posterior slope, weight-bearing on the tibia in a knee with CCL rupture creates shear forces, leading to abnormal tibial motion. The goal of TPLO surgery is to create a 3-7° slope on the tibial plateau (see Figure 8) that effectively controls tibial sliding by actively restraining the posterior cruciate ligament and the knee joint (see Figures 9 and 10). TPLO is an effective surgical procedure for dogs with complete and partial CCL ruptures.
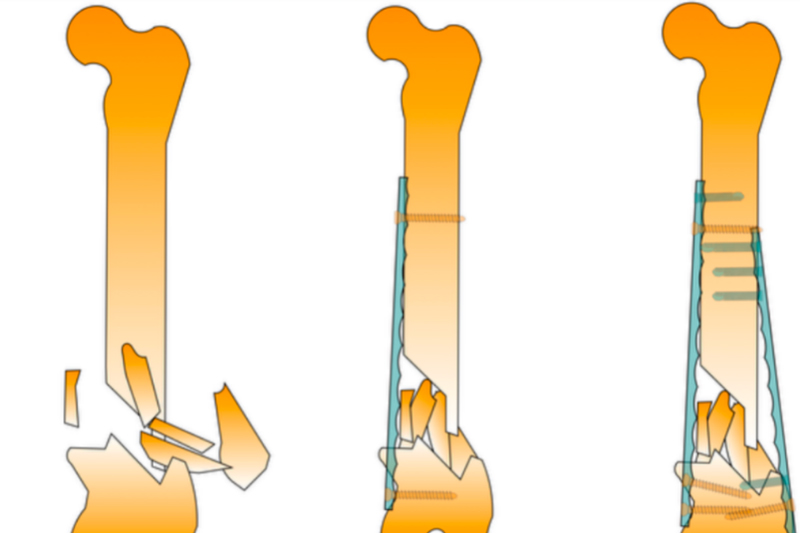
TPLO surgical steps:
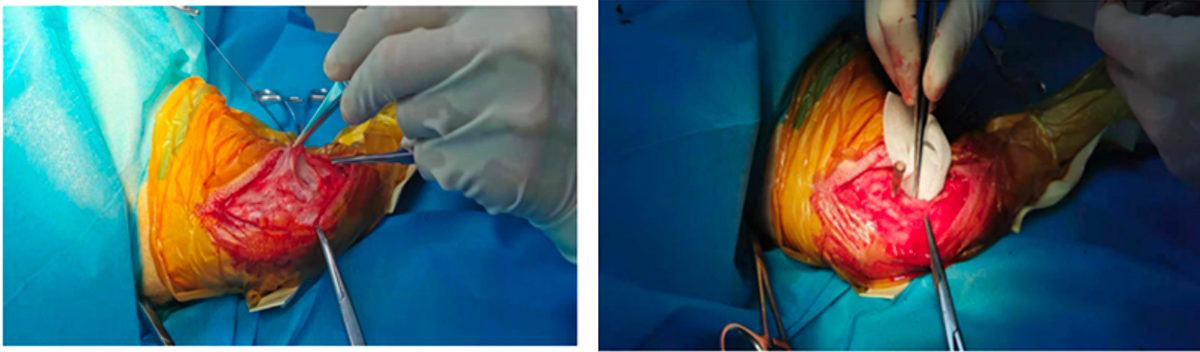
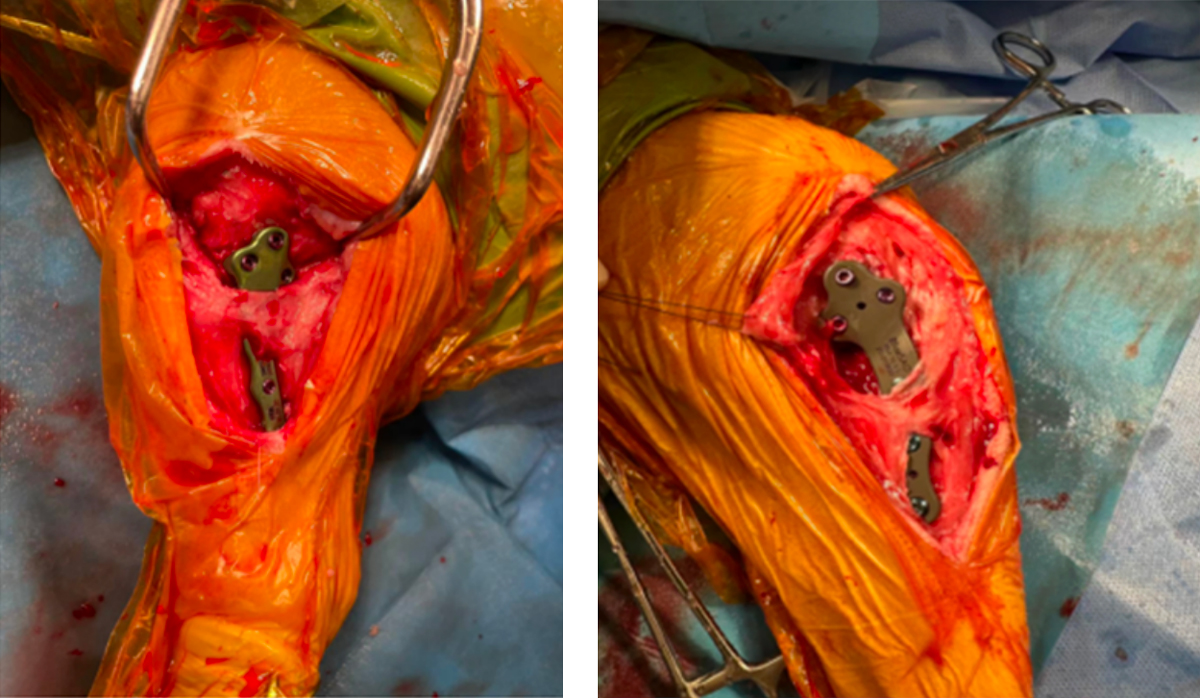
The proximal tibia is used as the surgical access point. The skin and subcutaneous tissue are incised to reveal the attachment of the anterior head of the sartorius muscle. The suture marks the insertion and the muscle is retracted posteriorly. A sharp incision is made at the origin of the popliteal muscle from the posterior tibia. The muscle origin is dissected from the medial edge of the posterior tibia. A moist gauze pad is placed between the muscle and bone to protect the muscle, popliteal artery, and vein . A 1mL syringe needle is inserted along the cranial aspect of the medial collateral ligament until it can be inserted perpendicularly into the joint capsule. This position is the center of the circular saw cut. Joint fluid should be observed at this point. In cases of degenerative disease, turbid joint fluid may be observed. A bone pry is inserted into the joint capsule and placed posterior to the straight ligament to protect it. A single layer of cortical bone is incised perpendicularly with the needle as the center. The rotation distance is carved out with an osteotome or electrocautery knife, and then a full-thickness incision of the rotated bone fragment is performed. Insert a Kirschner wire from the inner side of the proximal segment of the rotated bone block. This is the selection needle. Rotate it posteriorly to the marked distance. Insert a Kirschner wire from the head side of the tibial tuberosity as a temporary fixation needle. Then apply pressure with the TPLO pressure clamp and place the appropriate bone plate. The bone plate can be temporarily fixed with the Kirschner wire, and then the screws are tightened in sequence to complete the bone plate fixation. For very large dogs, auxiliary bone plate fixation is required. Use absorbable sutures to cross-suture the sartorius muscle, suture the deep fascia with the nodules, and suture the superficial fascia, subcutaneous tissue, and skin with the nodules.