



Feline spinal fractures
Abstract: In small animal clinical practice, spinal injury is a common cause of neurological dysfunction. Most common causes of spinal injury include disc herniation or dislocation, traffic accidents, falls from height, and bite injuries. Clinically, spinal injuries are most common in the thoracic and lumbar regions (T3-L3) and the lumbar and sacral regions (L4-L7). Spinal fractures can be treated with surgical, nonsurgical, or a combination of both.
Keywords: Spinal Injury
Case Description 1.
1.1 Basic Information: 8-month-old white female cat (Buji), intact, unneutered, unwormed, and unvaccinated, primarily fed cat food. 1.2 Chief Complaint: Normal in the morning before going outside. In the afternoon, she was found to be lowering her hind legs while walking. Soon, she was unable to stand upright on her hind legs, crawling on her belly. She was eating normally, eating what was brought to her mouth, and her bowel movements were normal. She lay motionless in her bed and cried out in discomfort when picked up
2.Clinical Examination
2.1 Physical Examination: She appeared to be in good spirits, responsive to external factors, and could move her head and neck normally. She was unwilling to walk, with her front limbs upright and her hind limbs constantly squatting. No obvious abnormalities were observed in the mucous membranes. No pain was detected on palpation of her limbs, and she could extend and retract them normally. Her respirations were approximately 50-60 breaths/minute, and her heart rate was regular and strong, at 160 beats/minute. Thoracolumbar palpation revealed significant pain at the thoracolumbar junction, with sensitive skin and muscles. Body temperature was 39.2°C, and weight was 3.5 kg. Cranial nerve examination revealed normal pupil size and light response, normal eyelid reflex, normal facial sensitivity, normal nasal sensitivity, no nystagmus, and normal masticatory muscles. 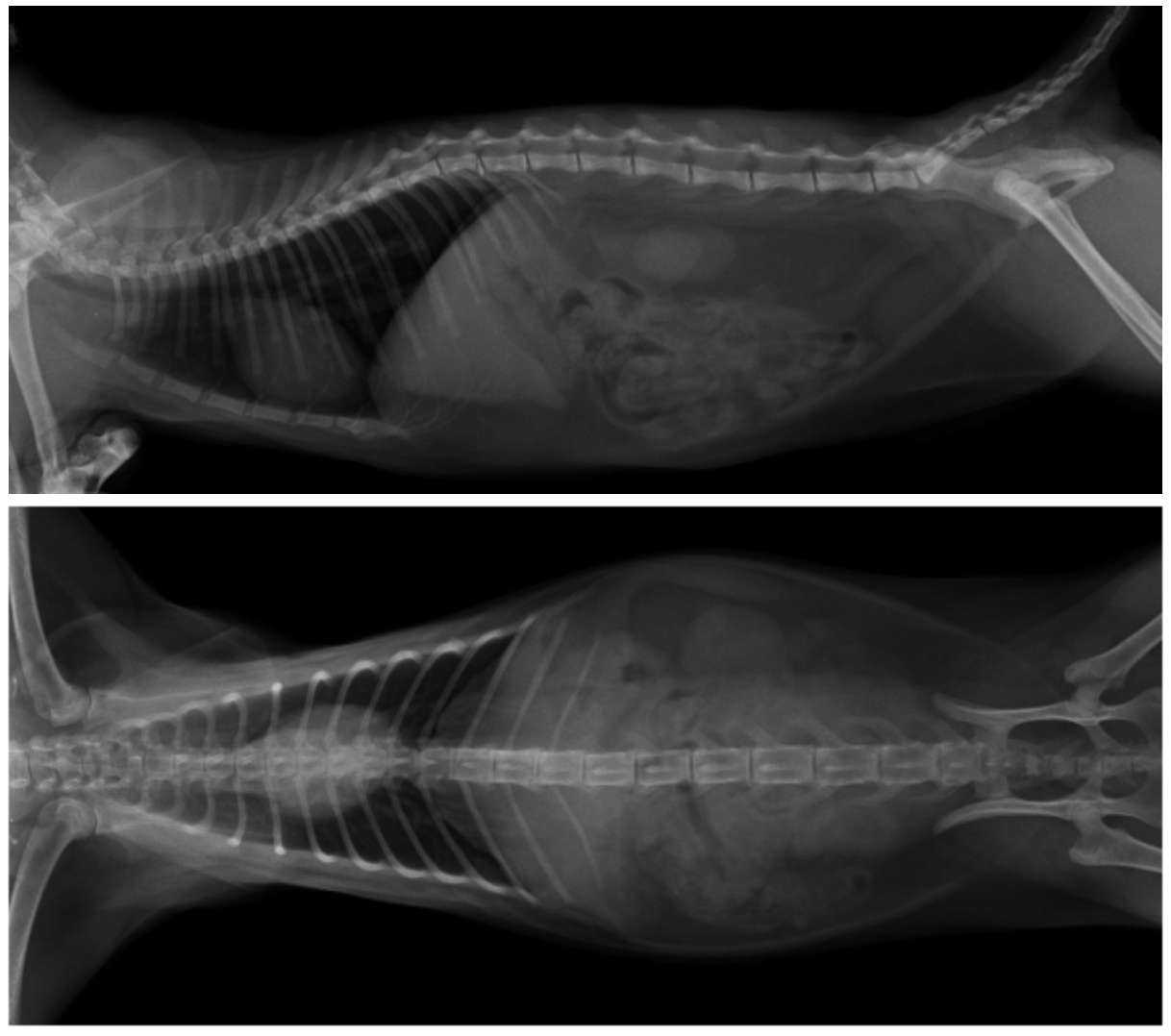
Figure 1 Preoperative CR image

Veterinary spinal pedicle screws
3. Diagnosis:
T12-T13 vertebral fracture. Treatment: Medical infusion therapy was administered on the first and second days.
1. 9% normal saline 40mlAmpicillin sodium 350mg/intravenous infusion.
2. 9% normal saline 40mlMethylprednisolone 15mg/intravenous infusion.
3. 9% normal saline 35mlMetabolic acid 3ml/intravenous infusion.
4. 5% glucose 30mlHuman albumin 2ml/intravenous infusion.
5. 10% glucose 30mlVitamin C 250mg/intravenous infusion.
6. Furosemide 10mg/subcutaneous injection.
Surgical treatment was performed on the third day:
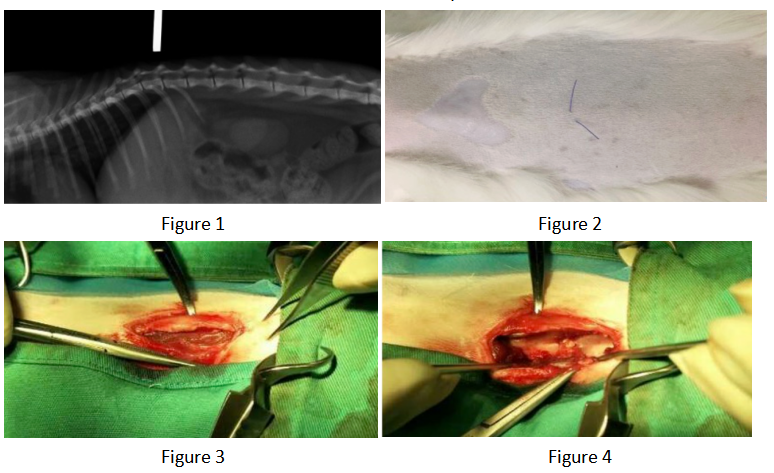
The hemilaminectomy site was redefined preoperatively based on plain X-rays (Figures 1 and 2). Surgical approach: A single incision of the skin and subcutaneous fat was made parallel to the dorsal midline, offset 1 cm (Figure 3). The lumbar multifidus muscle attached to each spinous process was exposed using a scalpel. The lumbar multifidus muscle was then bluntly dissected from the lamina using a periosteal elevator until it reached the facet articular processes (Figure 4). One or two articular processes were dissected in sequence, anterior and posterior to the affected area, and the surrounding tissue was completely separated from the bone to fully expose the articular processes. A rongeur was used to create a bite mark in the lamina anterior and posterior to the affected area, with repeated manipulations to deepen the mark. When cancellous bone was visible (Figure 6) and the dura mater was visualized, the rongeur was discontinued and replaced with a nucleus pulposus forceps, carefully removing the bone from the lamina to expose the medullary cavity. The rongeur and nucleus pulposus forceps were then used alternately to remove the affected articular processes, further exposing the medullary cavity (Figures 7 and 8). After the main surgery, the wound is irrigated, blood clots and bone fragments are removed, a fat pad is placed on the exposed medullary cavity, the lumbar muscles are repositioned, and the dorsal fascia is sutured. The skin tissue is closed routinely.

4. Recovery
The prognosis is good. He can walk and jump normally and is back to normal!

5. Sharing and Summary
This patient presented with normal physiological indicators at the time of presentation, considering that some injuries are not initially apparent. Furthermore, vertebral instability and displacement after a spinal fracture can lead to edema or hematoma in the surrounding tissues, further damaging the spinal cord. This can lead to energy metabolism impairment, lipid peroxidation, inflammation, and calcium channel disturbances at the injured site. Taking these factors into consideration, the patient was treated with intravenous fluid therapy that day, and the owner was advised that further evaluation would be necessary if his condition worsened. A high-dose of the glucocorticoid methylprednisolone was used. Methylprednisolone inhibits lipid peroxidation and inflammation, improves spinal cord blood flow after injury, prevents electrolyte imbalances within and outside the cells, and prevents spinal cord cell apoptosis. A diuretic was administered alongside intravenous fluid therapy to supplement nutrition, increase spinal cord blood flow, and raise arterial pressure. Diuretics increase urine output, allowing excess extracellular fluid to be removed from the injured tissue, thereby reducing pressure on the spinal cord from the edema. After two days of intravenous fluid therapy, Buji's spirits improved significantly, and he was able to eat, drink, and urinate normally. On the third day of presentation, a surgical hemilaminectomy was performed. Therefore, in addition to timely and effective spinal stabilization, relieving spinal cord compression, and decompressing the spinal cord, early medication is crucial. Medication can protect uninjured spinal cord tissue, reduce or prevent secondary injury, and promote nerve fiber regeneration. In spinal cord injury, early neurological examinations assess the localization of the lesion, the presence of multiple lesions, and the severity of the animal's nerve damage, all of which contribute to the patient's prognosis. The neurological injury grading scale is as follows: Grade 1 (pain only, hunched back, tight abdominal muscles, and a mostly normal gait); Grade 2 (moderate to severe pain, numbness, and leg weakness, but still able to walk); Grade 3 (numbness, uncoordinated movements, and paresis); Grade 4 (severe paralysis with possible incontinence and feeling in the legs); and Grade 5 (severe paralysis with no deep pain sensation). For severe cases of nerve damage grade 4 and above, the sooner surgical intervention is performed to remove mechanical compression, reduce edema, and relieve pressure, the higher the recovery rate.
6. Conclusion:
The animal recovered well through fluid infusion and fenestration to relieve spinal cord compression, achieving the desired effect.